



The development of Early Intervention (EI) services from a research-based clinical intervention into an integrated part of the health system was the theme of a symposium during the IEPA 10, held by the IEPA Early Intervention in Mental Health in Milan, Italy, from 20 to 22 October, 2016. Several leading specialists in EI presented their experiences, views and suggestions during the symposium.
Early intervention (EI) in psychosis is a comprehensive and evidence-based approach aimed at detection and treatment of psychotic symptoms in their early stages. Benefits are well documented and include a wide range of clinical, social and psychological outcomes for patients and their relatives. Patients spend less time with untreated psychosis, they have fewer symptoms, and they function better than those who receive standard treatments.
At the core of EI services is the concept of specialized assertive teams, in which staff members have a reduced caseload. These teams are multidisciplinary and include psychiatrists, psychiatric nurses, psychologists, social workers, employment support specialists and occupational therapists, among others. Clinical management is not restricted to pharmacological intervention, and other areas are likewise prioritised, including interpersonal problems, social skills, and vocational and educational issues.
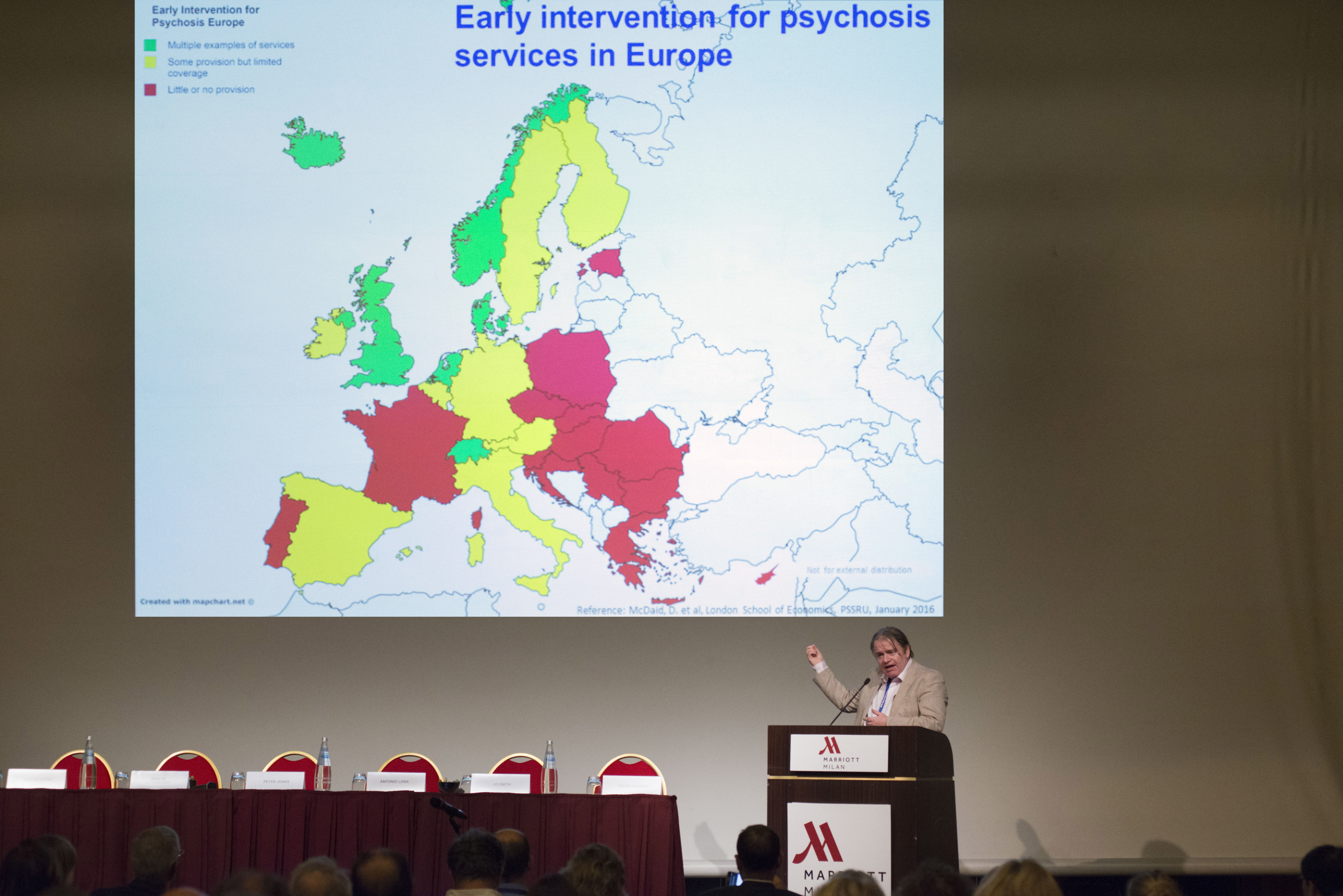
According to IEPA’s outgoing president, Masafumi Mizuno, from Toho University School of Medicine, Japan, there are examples of widespread implementation in the United Kingdom and Denmark, and in parts of Australia and Canada - but more is needed.
In England, a rapid increase in implementation of EI programmes occurred after 2001, promoted by a national policy implementation guide. But this widespread and policy-based dissemination and implementation of EI programmes became threatened. “After the financial crisis in 2008, managers had to save money”, explains IEPA’s president elect Peter B. Jones, from Cambridge University, UK. In the following years, over 50% of EI programmes in England had significant cuts in financing, adds Jo Smith, from the University of Worcester, UK. Fortunately, political efforts, sophisticated predicting tools, targeted funding and a system that reflects demographic and clinical differences helped to reverse the situation. “England is now in the second wave of system implementation”, says Jones. “Since April 2016, we have a new policy, in which a care coordinator should be allocated within two weeks, and this should be achieved in 50% of cases.”
A similar development can be seen in Denmark. “We have a good example of how EI was transferred from research to standard care”, says Merete Nordentoft, from the University of Copenhagen, referring to a landmark randomized study on EI, the OPUS trial. Since the initial positive results, EI services have been implemented over the whole country, thanks to promotion and public affairs, governmental starting grants, user involvement and efforts to maintain the services’ quality by continuous education and training of professionals. In 2016, experts and regional health authorities have agreed on a treatment package for people with psychosis. “If you have such a disorder, you are entitled to an evaluation within one month. This is a huge step”, she says.
In a different situation is Spain, where EI services have not yet been regularly implemented. “There are several reasons for this”, according to Celso Arango, from the University Hospital “Gregorio Marañón”, in Madrid. He points out that there is almost no coordination between mental health specialists, on the one hand, and primary care, welfare services or educational institutions on the other hand. Besides, he adds, there is a misbelief that mental health does not kill, and political interest is almost non-existing. “EI is mostly funded by research grants, and family associations contributes with funding and initiatives”, he completes. When asking other panellists what they would have done differently if they had campaign for early interventions all over again, representatives from the UK and Denmark mention organised public affairs campaigns and ensuring that the key messages reflected not only the evidence but also spoke to the heart of politicians.
David McDaid, from the London School of Economics, points out that pilot evaluation of different models of EI can make a difference where there is scepticism that these models can work. “It is also important to encourage collaboration with primary care services”, he says. But perhaps the most important is that clinicians should avoid thinking only in a clinical level. “Systems are important”, he sums up, referring to the mental health system, the primary sector, and wider social support systems.
Teresa di Fiandra, from the Italian Health Ministry, agrees. “We need to network with the educational system, the social sector and the labour sector”. She also cites user empowerment as a crucial approach. “But the most important take-home message for politicians is: try to invest more in the promotion and well-being of the population. We have already done a lot of work assessing the evidence, we need to move to real action”, she says. In her department, she exemplifies, there is a funding mechanism that prioritises research that is immediately applicable to the national health system. “A central governmental office can also, as we do, provide a framework and promote continuous monitoring of services”.
Factors that contributed to the implementation of EI services varied according to cultural and organizational aspects in each country, but user participation, users’ narratives, and known personalities that embrace the cause are frequently present, summarizes the leaders of these successfully implemented EI programmes. Clinicians might also partner with people that have the expertise and skills to show the economic value of EI to politicians and to promote change in health systems. More good advice includes increased focus on user and community involvement and on a broader systemic approach.
There is also some reason for optimism in regions that struggle to implement EI in health systems. “Implementation of EI programmes can move very quickly”, says Peter B. Jones, who describes the initial developments in Australia and Europe as “sending humans to the moon”, but compares the progress during the past four years in the United States, where over 100 EI services will soon be operating, to “building a space station on Mars”.